Try our playground on desktop
We'll send you the link to try there.
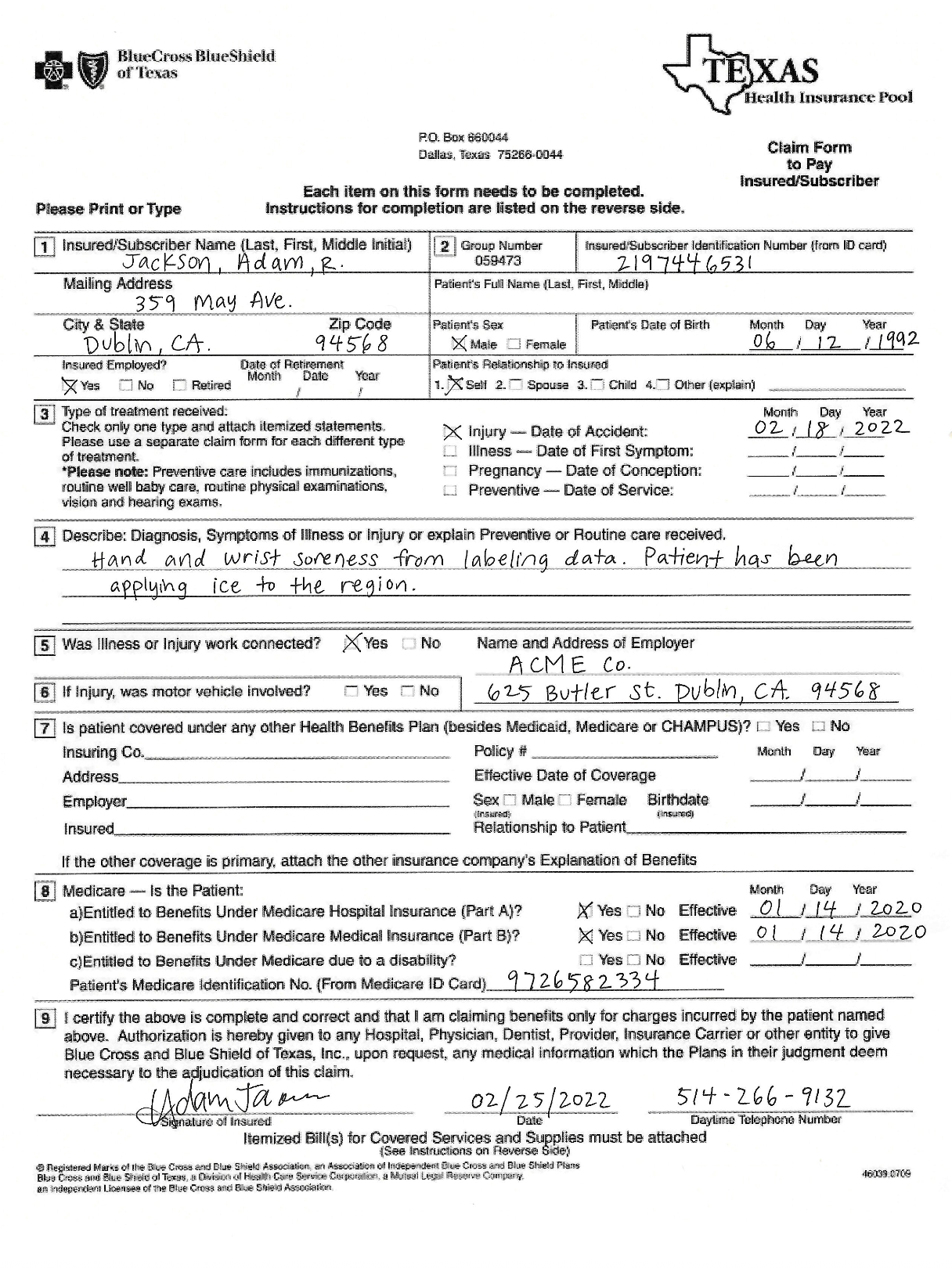
BlueCross BlueShield of Texas
Please Print or Type
P.O. Box 66064
Dallas, Texas 75266-0044
Each item on this form needs to be completed.
Instructions for completion are listed on the reverse side.
TEXAS Health Insurance Pool
Claim Form to Pay
Insured/Subscriber
Insured/Subscriber Name (Last, First, Middle Initial): Jackson, Adam, R. Group Number: 059473 Insured/Subscriber Identification Number (from ID card): 2197446531 Mailing Address: 359 May Ave. City & State: Dublin, CA. Zip Code: 94568 Patient's Full Name (Last, First, Middle): Patient's Date of Birth: Month: 06 Day: 12 Year: 1992 Patient's Sex: [x] Male [ ] Female Insured Employed?: [x] Yes [ ] No [ ] Retired Date of Retirement: Month: / Date: / Year: / Patient's Relationship to Insured: [x] Self [ ] Spouse [ ] Child [ ] Other (explain)
Type of treatment received: Check only one type and attach itemized statements. Please use a separate claim form for each different type of treatment. *Please note: Preventive care includes immunizations, routine well baby care, routine physical examinations, vision and hearing exams. [x] Injury - Date of Accident: 02 / 18 / 2022 [ ] Illness - Date of First Symptom: / / [ ] Pregnancy - Date of Conception: / / [ ] Preventive - Date of Service: / /
[x] Describe: Diagnosis, Symptoms of Illness or Injury or explain Preventive or Routine care received: Hand and wrist soreness from labeling data. Patient has been applying ice to the region.
Was Illness or Injury work connected? [x] Yes [ ] No Name and Address of Employer: ACME Co. 625 Butler st. Dublin, CA. 94568 If Injury, was motor vehicle involved? [ ] Yes [ ] No Is patient covered under any other Health Benefits Plan (besides Medicaid, Medicare or CHAMPUS)? [ ] Yes [ ] No Insuring Co. Policy # Address Effective Date of Coverage: Month / Day / Year Employer Sex: [ ] Male [ ] Female Insured Birthdate: Month / Day / Year Relationship to Patient If the other coverage is primary, attach the other insurance company's Explanation of Benefits
Medicare - Is the Patient: a) Entitled to Benefits Under Medicare Hospital Insurance (Part A)? [x] Yes [ ] No Effective 01/14/2020 b) Entitled to Benefits Under Medicare Medical Insurance (Part B)? [x] Yes [ ] No Effective 01/14/2020 c) Entitled to Benefits Under Medicare due to a disability? [ ] Yes [ ] No Effective Patient's Medicare Identification No. (From Medicare ID Card) 9726582334
[x] I certify the above is complete and correct and that I am claiming benefits only for charges incurred by the patient named above. Authorization is hereby given to any Hospital, Physician, Dentist, Provider, Insurance Carrier or other entity to give Blue Cross and Blue Shield of Texas, Inc., upon request, any medical information which the Plans in their judgment deem necessary to the adjudication of this claim. Signature of Insured: Adam Jamon Date: 02/25/2022 Daytime Telephone Number: 514-266-9132 Itemized Bill(s) for Covered Services and Supplies must be attached (See Instructions on Reverse Side)
d) Registered Marks of the Blue Cross and Blue Shield Association an Association of Independent Blue Cross and Blue Shield Plans
Blue Cross and Blue Shield of Texas, a Division of Health Care Service Corporation 9 Mutual Legal Reserve Company
an independent Licensee of the Blue Cross and Blue Shield Association
46039.0709